
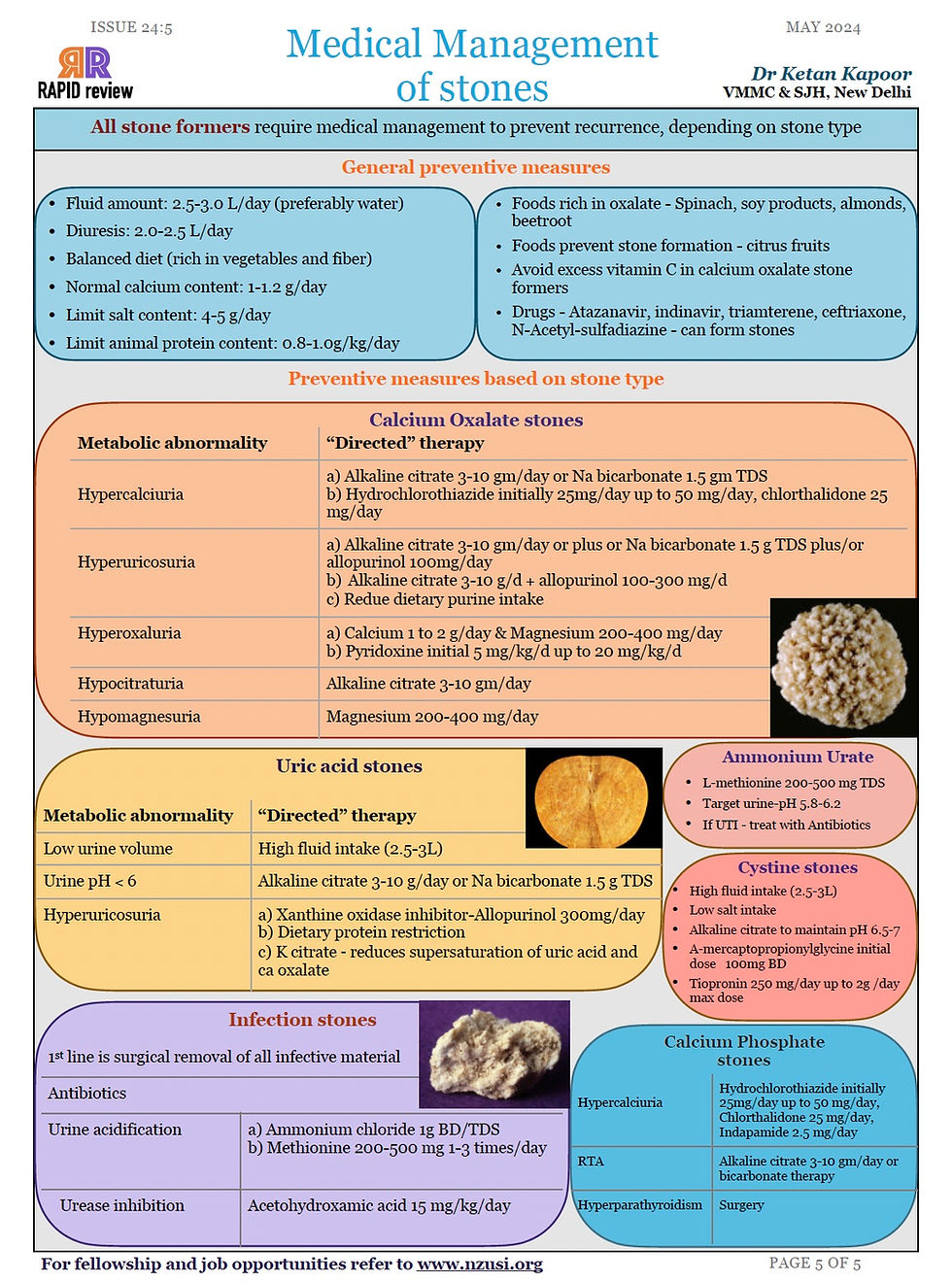
Medical Management of Renal Stones
- May 6, 2024
- 1 min read
Dr Ketan Kapoor, VMMC & SJH, New Delhi
General Preventive Measures
Fluid amount: 2.5-3.0 L/day (preferably water)
Diuresis: 2.0-2.5 L/day
Balanced diet (rich in vegetables and fiber)
Normal calcium content: 1-1.2 g/day
Limit salt content: 4-5 g/day
Limit animal protein content: 0.8-1.0g/kg/day
Foods rich in oxalate - Spinach, soy products, almonds, beetroot to be avoided
Foods prevent stone formation - citrus fruits
Avoid excess vitamin C in calcium oxalate stone formers
Drugs - Atazanavir, indinavir, triamterene, ceftriaxone, N-Acetyl-sulfadiazine - can form stones.
Calcium Oxalate Stones
Metabolic abnormality | “Directed” therapy |
Hypercalciuria | a) Alkaline citrate 3-10 gm/day or Na bicarbonate 1.5 gm TDS b) Hydrochlorothiazide initially 25mg/day up to 50 mg/day, chlorthalidone 25 mg/day |
Hyperuricosuria | a) Alkaline citrate 3-10 gm/day or plus or Na bicarbonate 1.5 g TDS plus/or allopurinol 100mg/day b) Alkaline citrate 3-10 g/d + allopurinol 100-300 mg/d c) Redue dietary purine intake |
Hyperoxaluria | a) Calcium 1 to 2 g/day & Magnesium 200-400 mg/day b) Pyridoxine initial 5 mg/kg/d up to 20 mg/kg/d |
Hypocitraturia | Alkaline citrate 3-10 gm/day |
Hypomagnesuria | Magnesium 200-400 mg/day |
Uric Acid stones
Metabolic abnormality | “Directed” therapy |
Low urine volume | High fluid intake (2.5-3L) |
Urine pH < 6 | Alkaline citrate 3-10 g/day or Na bicarbonate 1.5 g TDS |
Hyperuricosuria | a) Xanthine oxidase inhibitor-Allopurinol 300mg/day b) Dietary protein restriction c) K citrate - reduces supersaturation of uric acid and ca oxalate |
Infection stones
1st line is surgical removal of all infective material | |
Antibiotics | |
Urine acidification |
Figure 1: Medical Management of renal Stones



Comments